January 12, 2016: Backboards, Family Presence, and Tox
WE FINALLY HAVE SOME VIDEOS!
WALT LUBBERS: Why the hell are we still talking about backboards?
The evidence for prehospital "spinal immobilization" is non-existent, but the harms are well documented. The long spine board is great as a lifting or extrication tool, but as soon as the lifting or extrication is over, their benefit ends and their harm rapidly ensues. Cervical collars do limit visible motion of the spine, but there is again no evidence for a patient-centered benefit, and striking evidence that application of a cervical collar either does nothing (see every trauma patient who comes in in a no-neck size rigid collar) or causes harm. The backboard is there to give patients handles, and the collar is there to remind them not to wiggle their head around (not that someone with an actual spine injury would because it hurts). The adoption of a soft collar, sungging the patient to a padded stretcher, and use of a vacuum mattress if they can't hold still is the Third Path to EMS enlightenment.
PATTI HOWARD: Family Presence During Resuscitation
As we contemplate the path to enlightenment, we eventually realize that most of what we think we got into this for (ie save people from cardiac arrest) actually won't make a difference; everyone dies eventually, and most of the time we're unable to stop that process. So we need to recognize that when a family calls us to the side of a patient in arrest, we often don't make a difference for the patient, but we can make a huge difference for those that are left behind. Most of the time, the family won't interfere with efforts, and are grateful to see you working so hard to do what you can for their loved one. While resource constraints often limit what we can do, we should develop the expectation and culture of including the family (if they desire) in what are likely a patient's last moments. So stay on scene for your resuscitation, and once you have the airway managed, someone doing CPR, and have a couple of pulse checks under your belt, peel someone off and talk to the family (IMO, preferably the lead provider, but an officer, a BC, or whoever is best at talking to families, whether medic or EMT will work just fine).
WCL (personal note): Like teenagers and sex, I have found that most families do better if they know what is happening and what to expect than if they learn about it off the TV.
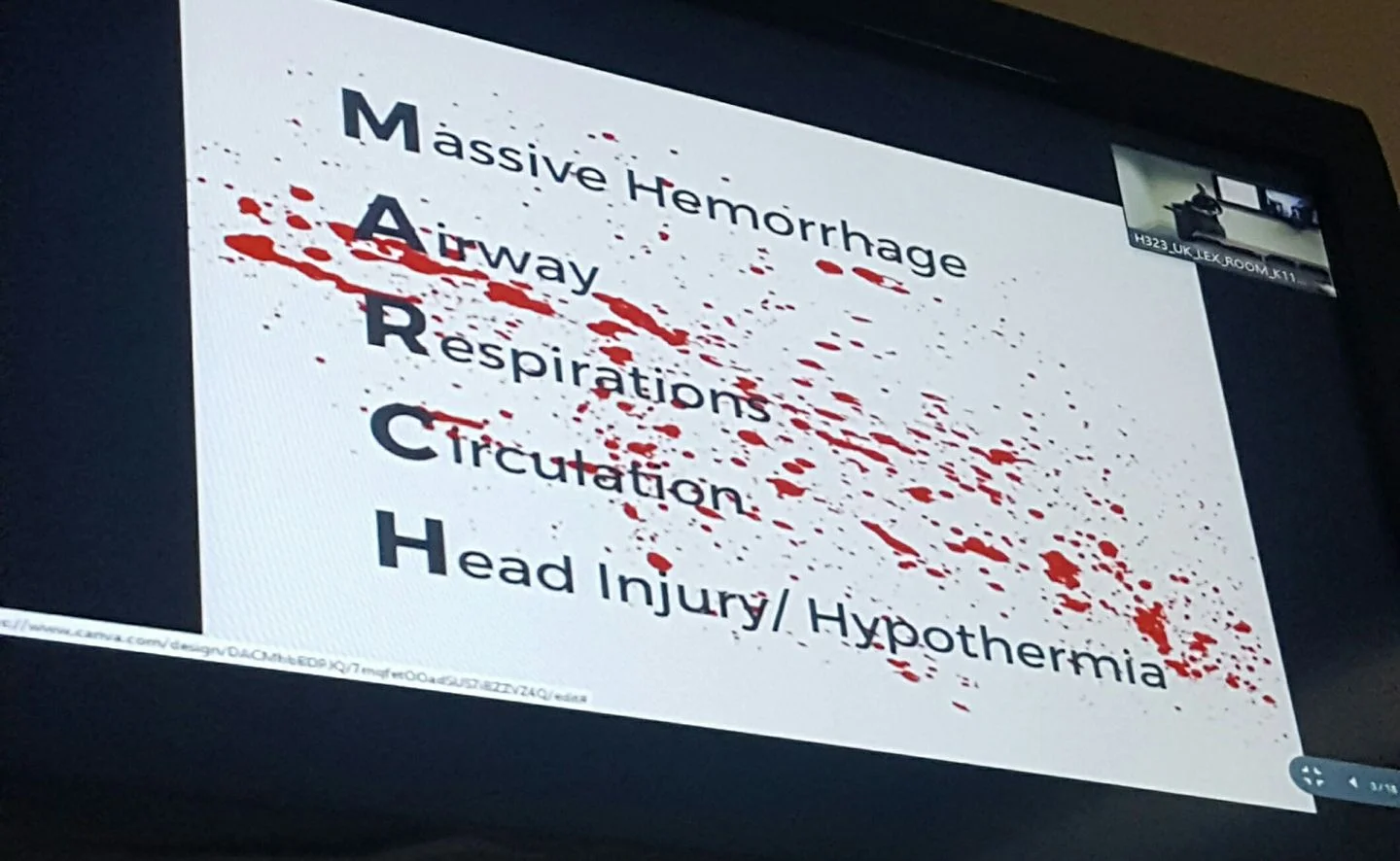
IAN BOYD AND JON VIVOLO: Tox on the Run
There's some basic stuff you need to know about toxicology, and some basic things you can do for most cases. There's very little tox wise that doesn't respond to supportive care, so even if you don't know they took, Airway-Breathing-Circulation is a pretty reasonable mantra. You should have Poison Control on speed dial-
1-800-222-1222
Don't forget that you should protect yourself above all else (compelling video here: https://www.youtube.com/watch?v=znQwAcOQffQ).
There are some "mystery" cases that actually are easily explained toxicologically. Beware that vape-ing liquid (ie nicotine) is widely available, has poor oversight/ regulation/ quality control, and that children may ingest a toxic or lethal dose in a single mouthful. Symptom onset is bimodal, with initial symptoms within minutes (agitation), generalized convulsions etc potentially an hour later. Carbon monoxide makes oxygen stick to your hemoglobin but won't release to your cells, so O2 sat may be 100% but your cells may think it's 50% (made that number up). If the whole family including the dog suddenly gets stomach flu one morning, be really suspicious of CO. Give lots of O2.